So, it finally happened. You have bitch tits. The infamous gynecomastia. You’ve heard stories of it, you’ve seen it, you knew this day will come, but you — just like pretty much all men — were not prepared.
No panic. We’ve got you covered. Here’s how you get rid of gyno, what are your chances to avoid surgery, and everything you should know about it.
The Basics of Gyno
First of all — let’s make sure that we’re on the same ground. Are you even sure you have gynecomastia, and your chest is not just fat?
What is Gynecomastia?
In medical terms, it’s an increase in breast gland tissue in men. You, just like all men, have SOME gland tissue there, but the amount is miniscule. When it gets bigger — it means that you’ve triggered gyno.
It manifests because of hormonal imbalance:
- Estrogen is too high;
- Testosterone is too low;
- IGF-1 is too high (by itself exogenously, from Growth Hormone, or from MK-677, a SARM also known as Ibutamoren);
- Or prolactin is not at its normal level.
Some argue that gyno can be triggered by prolactin alone, some say that it depends on your estrogen levels only. We see it more as a combination of these factors.
You’ll never get gynecomastia if your prolactin is slightly above the normal level, while your estrogen and Testosterone are perfectly good. And you won’t get it from a minimal increase in e2 (estradiol) if your prolactin, IGF-1 and Test are OK.
However, since we’re talking about gyno that you — most likely — caused by your a bit too enthusiastic use of steroids, the primary reason should be high estrogen.
To put it simply, when you introduce exogenous testosterone, your body converts a portion of it into estrogen via the aromatase enzyme. If estrogen levels exceed what your androgen receptors can balance, excess estrogen binds to receptors in breast tissue, stimulating gland growth.
What causes it?
Another common reason for gyno might be just puberty. In this case, relax and enjoy the ride: it will, as it does in most cases, disappear by itself.
During puberty (ages 12-16), hormonal fluctuations—especially ratio changes between testosterone and estrogen—can temporarily cause gynecomastia. In most cases, this resolves on its own within 6 months to 2 years.
Sadly, puberty and steroids are not the only things that can trigger moobs. And we say «sadly» because you can always drop steroids (slowly and with PCT, of course), but you can’t drop other causes, like:
- Tumors in your adrenal glands or testes;
- Chronic kidney issues;
- Hyperthyroidism;
- Cirrhosis or other liver issues.
Gynecomastia may not be the main problem (after all, it’s just a cosmetic issue) if it’s caused by one of these nasty things. They’re way more dangerous for your health than a few grams of extra gland tissue behind your nipples.
We suggest a medical check if you have reasons to believe that you have one of these. Maybe you need to focus on the cause of the issue, and not cosmetic stuff, like gyno.
Gynecomastia Symptoms
Now — how exactly did you find out you have gyno? And how can you be sure that you have it? It’s more than possible to miss early symptoms of gyno:
- Increased nipples sensitivity;
- Puffy, slightly “swollen” nipples;
But it’s impossible to miss it when it develops further:
- Visibly enlarged breasts;
- Lumps under the skin you can feel and touch.
That’s it. The primary symptoms are physical: nipple sensitivity, puffiness, visible enlargement, and palpable lumps. Gyno itself doesn’t cause fever or systemic illness—but the hormonal imbalance behind it can affect mood and energy levels.
How to Deal with Gynecomastia
Now that you’ve checked and you’re 99% sure you have gyno — how do you deal with it? Let’s go step by step on your road back to a normally looking chest.
Step 1: No Panic, No Depression
Gyno is reversible, it’s not here to stay, and even — in the worst case — if you will have to remove it surgically, it’s not the worst operation in existence. You’re going to be OK.
Studies show that gynecomastia causes significant psychological distress in the majority of affected men—with some research indicating that over 80% report embarrassment or anxiety about their condition.
Gynecomastia is known to cause:
- Depression;
- Mood swings;
- nervousness;
- Sociophobia;
- Anxiety.
NONE of these mental side effects manifest directly. It’s all because some guys become self-conscious, can’t stop looking at their newly-developed moobs, and go on a whining self-pitying rampage. Please remember:
Your bitch tits should not make you act like a bitch. You’re a man with moobs, not a girl with balls.
Go on with your lifestyle. Don’t be afraid to show up in public. Keep working out. Keep your diet spot on. Don’t let something as petty as tiny man boobs affect your life.
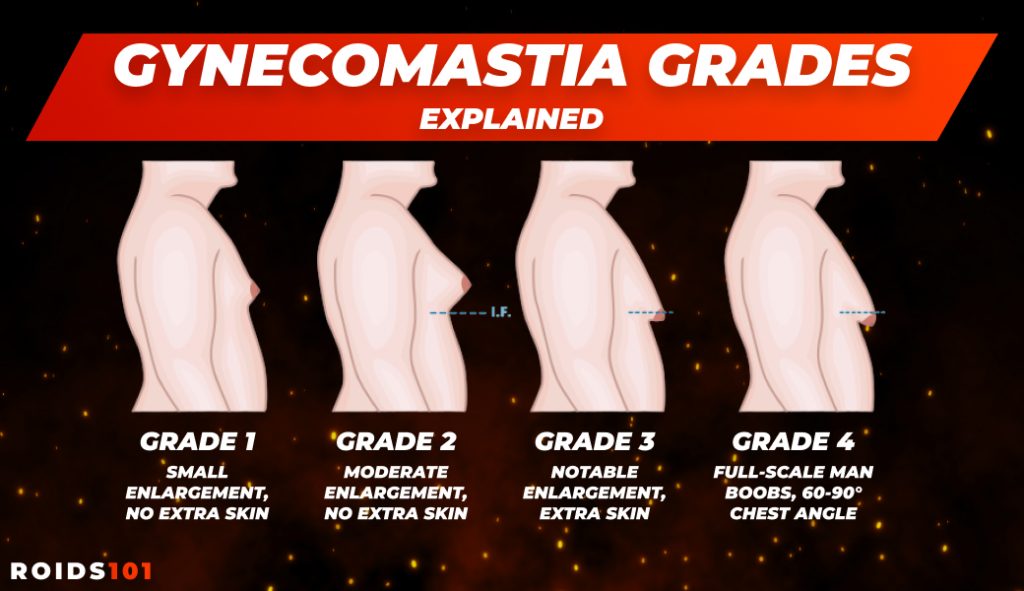
Step 2: Get to Know Your Enemy (Gynecomastia Grades)
Now that you’re ready for the fight, let’s observe the problem. How bad is it really?
We have 5 main gynecomastia grades:
- Grade 1 — Small enlargement, no extra skin (basically, you can feel something UNDER your nipples, and your nipples get more sensitive, but it does not look like, well, a boob);
- Grade 2a — Moderate enlargement with no extra skin (something under your nipple is rather big, it’s not just a tiny lump, it fills the whole area under lower chest muscles);
- Grade 2b — Moderate enlargement with some extra skin (same size as grade 2a, but it’s not on the inside, and it’s visibly popping out);
- Grade 3 — Marked enlargement with extra skin (this grade looks like a female breast, your skin has grown to keep it, and it barely fits in your palm);
- Grade 4 — Marked enlargement, 60-90 degree chest angle (full-scale moobs that HANG from your chest, not just pop out).
The good news is — you will, most likely, catch it early, at grade 1 or 2. These are the most popular ones.
Note that not just the size, but also — the density of lumps under your skin plays a big role: the softer it is — the more chances you have to get rid of it with n surgical intrusion.
Step 3: Fight Back (Gynecomastia treatment)
Now — time to fight back. You have 3 major ways to go:
- Tamoxifen (Nolvadex);
- Raloxifene (Evista);
- Surgery.
Both are SERMs (Selective Estrogen Receptor Modulators), and you surely know Nolva as one of the most popular PCT compounds in existence.
Blocking the estrogen receptors is exactly what you need: no estrogen will be able to “connect” to your breasts, they’ll stop growing and will start slowly disappearing.
Tamoxifen Dosage with Gynecomastia
With Tamoxifen, you don’t need A LOT to fight gyno. In this study on Nolvadex vs gynecomastia, doses as low as 10-20mg ED were proven to be effective. So it’s really simple:
Start with 10mg every day, up the dose to 20 if it doesn’t work at all in 2-3 weeks.
Some older studies explored various dosing protocols, but the current medical consensus and bodybuilding experience both support daily dosing (10-20mg ED) as the most reliable approach for existing gynecomastia.
Raloxifene Dosage with Gynecomastia
Raloxifene is a Second generation SERM, but it’s in the same class as Nolva. It’s more effective, more powerful, but has poor bioavailability.
In short, your body destroys and digests most of it before it can make any difference and make it to the target area. That’s why Raloxifene doses are significantly higher:
Start with 50-60mg ED, it will leave gyno no chances in 3-9 months.
Both Nolva and Raloxifene are generally well-tolerated at therapeutic doses, but they’re not side-effect-free. Possible effects include hot flashes, leg cramps, and—rarely—more serious issues like blood clots. Always consult a healthcare provider before use. Most importantly — both are proven by multiple studies to be effective in countering gyno.
Gynecomastia Removal Surgery
This is your last option. Just remove the whole gland tissue and get your normal chest appearance back. It is, of course, a little controversial:
The Pros:
- You get your gyno removed fast;
- The result is guaranteed;
- No extra pressure on your body and hormones.
The Cons:
- It’s pricey;
- You get your nipple area sliced, lifted, and some pieces of your body removed. It’s a God damn full-scale surgery;
- Risk of infections if the clinic makes a mistake;
- You’ll need anesthesia—which carries standard surgical risks but is generally safe for healthy adults when administered by qualified professionals;
- You skip at least some chest days in the gym;
- And you may or may not have scars on your chest, depending on the doc’s professionalism and your age.
The final decision is — of course — up to you. We’d recommend leaving the surgical intrusion for the worst case scenario and at least try to fight back with SERMs first.
Step 4: Make Sure it Never Comes Back
In case you remove your gyno surgically — it has no chances to come back, ever. However, if you go the Tamoxifen or Raloxifene way, you’ll have to prevent moobs from coming back ever again. Here’s what you can do:
- Keep your damn doses of gear low;
- Keep your PCT on God damn point and don’t skip it;
- Add AIs (Aromatase Inhibitors) on cycle, you don’t need extra estrogen.
Be cautious with aromatase inhibitors: excessive doses can crash estrogen too low, causing joint pain, libido loss, and mood issues. Estrogen plays important roles in bone health and cognition—you don’t want zero estrogen, just balanced levels. Just keep the dosage on point, “the more the better” approach NEVER works in bodybuilding.
Step 5 and Conclusion: Just Chill
This is the final step. Gynecomastia is not some nightmarish incurable illness. It’s literally just bitch tits. Not even big enough in the majority of cases to make wearing BRAs mandatory.
If caught early and treated properly, gynecomastia often resolves within 3-12 months. However, once breast tissue becomes fibrotic and hard (typically after 12+ months), it rarely responds to medication and may require surgical removal
Just do your best to avoid it (because moobs look worse than a nice, dry and shredded chest), but if it ever comes — don’t panic. Just fight back.
Gynecomastia Treatment Options Comparison: SERMs vs Surgery vs AI
When gyno hits, you need to act fast—but you also need to act smart. Different situations call for different approaches. Here’s a complete breakdown of every gynecomastia treatment option available in 2026, so you can choose what actually fits your case.
| Treatment | Best For | Time to Results | Success | Cost | Key Risks |
| Tamoxifen (Nolvadex) | Early gyno | 4–12 weeks | 70–80% | Low | Mild hormonal sides |
| Raloxifene (Evista) | Early or Nolva-resistant gyno | 6–16 weeks | 80–90% | Moderate | Mild cramps, hot flashes |
| Aromatase Inhibitors | Prevention on cycle | 1–3 weeks | High (prevention) | Low–Moderate | Low estrogen symptoms |
| Cabergoline | Prolactin-related gyno | 2–6 weeks | ~80% | Moderate | Nausea, dizziness |
| Letrozole | Severe high estrogen | 3–7 days | Very high | Low | Estrogen crash |
| DIM / D-Glucarate | Mild prevention | 4–8 weeks | Low | Low | Minimal |
| Surgery | Advanced gyno | Immediate | 95%+ | Very high | Scarring |
| Liposuction | Fat-only chest | Immediate | ~90% | High | Bruising |
| Wait | Puberty cases | 6–24 months | ~50% | Free | May persist |